US Cardiac electrophysiologists meet reimbursement reality and don’t like it.
0 View

- Publish Date:
- 2 August, 2022
- Category:
- Herbs
- Video License
- Standard License
- Imported From:
- Youtube
By ANISH KOKA
It’s been a while but Anish Koka, a one time regular writer on THCB and occasional THCB Gang member, is back publishing up a storm on his Substack channel. You may recall that his political and clinical views don’t always mesh with some of the wooly liberals we feature on THCB (cough, cough, me), but we are delighted to be back publishing some of his pieces–this one is on reimbursement.–Matthew Holt

The subspecialty of Cardiology known as electrophysiology has seen explosive growth over the last few decades in large part because of a massive expansion in the suite of procedures now offered to patients. It used to be that electrophysiologists would spend the majority of their careers implanting pacemakers and defibrillators, but the last 2 decades saw an explosion in electrophysiology procedures known as ablations. Ablations essentially involve burning cardiac tissue in a strategic manner to get rid of arrhythmias that may be afflicting a particular patient. The path humans took from first taking an electrical picture of the heart with a surface ECG to putting catheters into the heart to map and treat dangerous arrhythmias is one of the great achievements of the modern era.
Giants of the field like the recently deceased Mark Josephson essentially created a field by going where no humans had gone before. Dr. Josephson did much of his work in Philadelphia at the University of Pennsylvania publishing seminal papers that lead to a greater understanding and eventual treatment of previously incurable malignant arrhythmias. As is true of all trailblazing work in medicine , there were no reimbursement codes in the beginning , just desperate patients with no place to turn.
The procedures being embarked on were rare and the patients were very complex. The renumeration that was awarded from Medicare was reflective of this. But two things almost always happen once a highly reimbursed procedure code comes on line – technological advances makes the procedure easier, and the population that the procedure is intended for massively balloons.
Campaigns are launched to educate patients about the disease they may be carrying, physicians are inundated with educational material about the importance of screening their unsuspecting patients that may need CPT code 973443 (that’s made up), and somehow, inexorably, the evidence base shifts to suggest ever milder versions of a disease needs treatment.
Ablation for an exceedingly common arrhythmia – atrial fibrillation – takes this exact course. Initially an arduous procedure that was only meant for the worst, most symptomatic patients, has now evolved to be offered to even mild patients.
This would explain why the executive I spoke to who told me of his executive physical program that involved him flying to one of our great academic medical centers for a battery of tests yearly. One year, he was discovered to have atrial fibrillation incidentally. He thanked his stars the crack team had quickly arranged an ablation for him. He felt ‘great’ and ‘blessed’.
It turns out that a well reimbursed procedure code is the equivalent of striking gold. The gold rush that follows consists of a motley crew of health systems large and small anxious to cash in. The winner is the individual who can bill the most codes in one day. In this world, speed trumps quality. Academic medicine in the not so distant past used to be insulated from these incentives because payments to employee physicians weren’t tied to clinical or procedural volume. Those days are long gone. Compensation almost everywhere is now tied to the number of Relative Value Units (RVUs) that a physician can ‘produce’.
RVUs are determined by Medicare, and define the value of a service or procedure relative to all services and procedures. This measure of value is based on the extent of physician work, clinical and nonclinical resources, and expertise required to deliver the healthcare service to patients. RVUs can be roughly converted to reimbursement when a conversion factor (CF), dollars per RVU, is applied to the total RVU.
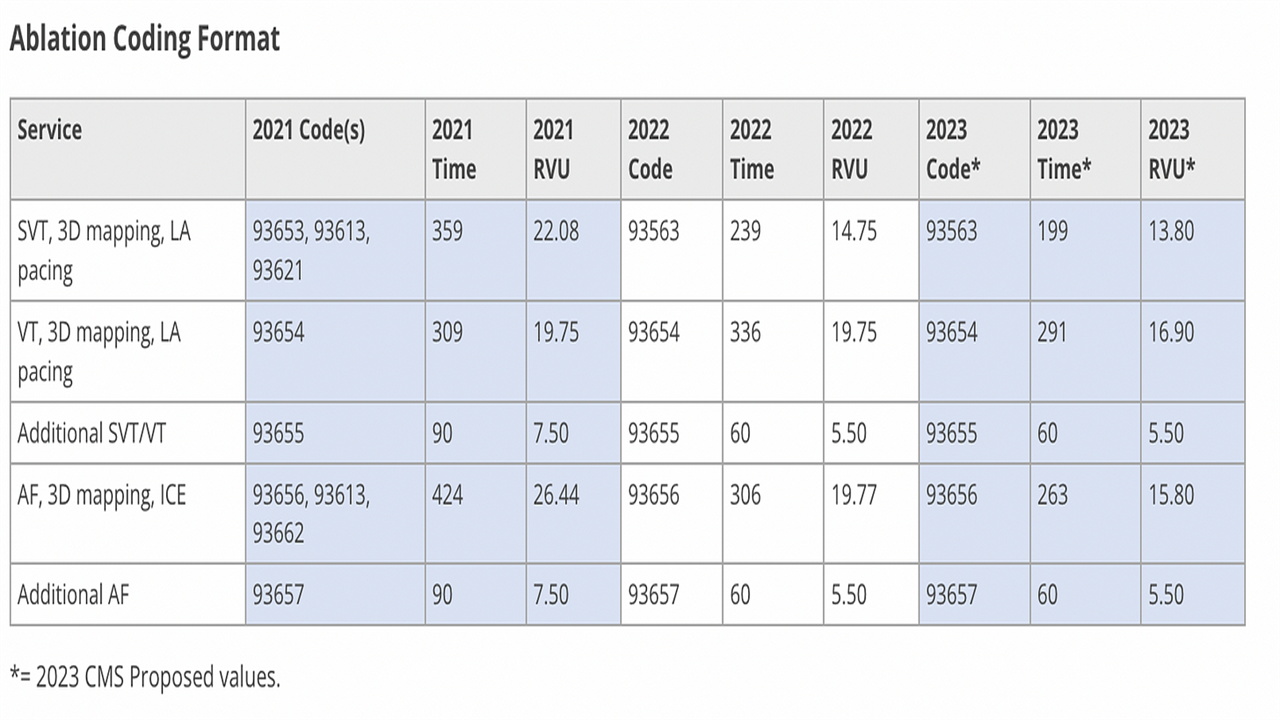
Because the amount of time taken to do a procedure isn’t stable over time, Medicare performs a yearly assessment via surveys of physicians. In the case of ablations, surveys of electrophysiologists executed by professional organizations in the fall of 2020 demonstrated notable reductions in procedure times. These surveys were redone in 2021 and reconfirmed significant reductions in procedure times. The American Medical Association/Specialty Society RVS Update Committee (RUC) which makes recommendations to Medicare attempted to make the case that time should not be the sole factor in the determination of reimbursement and recommended higher RVUs.
While a reduction in time does imply a reduction in work it is not the position of the ACC that this change is a nearly absolute 1 to 1 ratio. As procedure times are reduced the intensity of the work is not necessarily reduced by the same amount and can in fact result in an increase in intensity of the work. This is part of the reason why the RUC-recommended RVUs were not precisely correlated with the reduction in time.
These pleas have, so far, fallen on deaf ears. Medicare’s cuts basically approximate the reduction in time percentage noted in the clinician surveys.
Medicare has its own motivations of course. The Medicare trust fund has been teetering on the brink of insolvency for some time now, and part of staving off bankruptcy is engaging in a game of wack-a-mole with regards to new, expensive, high volume procedures.
Electrophysiologists apparently thought they were immune from this basic reality. The level of hysteria in response to these procedural reimbursement cuts is especially remarkable given the wide spread support of many physicians for economic mitigation policies over the COVID years that have only made things worse.
Medicare revenues were dramatically affected by COVID-19 because the amount of payroll taxes expected to flow into the trust fund was reduced due to the pandemic’s economic effects, and testing and treatment costs for the virus. Additionally, several pieces of legislation and policy increased spending, including payments for COVID-19-related inpatient admissions being hiked by 20% and an expansion of tele-health funding.
Money doesn’t grown on trees, and physicians that have enjoyed the benefits of a third party financing of healthcare are in for a rude awakening if the third party (the American taxpayer) runs out of money. There is most certainly a better path to travel for patients and physicians, but so far at least, physicians mostly seem content to throw tantrums about their worth not being recognized by society on twitter.
This wouldn’t be a winning strategy in normal times, but for those who comprise the top of the income scale within the physician community to complain about cuts that appear in line with the reduced time and complexity it now takes to do these procedures while the average American struggles to pay grocery and gas bills seems in particularly poor taste.
Anish Koka is a Cardiologist. Subscribe to his Substack and follow him on Twitter at @anish_Koka













