13 Year Old McAllen
0 View

- Publish Date:
- 14 February, 2023
- Category:
- Holistic
- Video License
- Standard License
- Imported From:
- Youtube
BY IAN MORRISON
As a Scot, obviously I am a whisky fan, and although I prefer the smoky malts of Islay (where my grandfather was from and where I visit my friends there frequently), I am also a huge fan of McCallan 18-year-old whisky, the sticky toffee pudding of single malts.
But as all policy wonks know, McAllen Texas is not famous for whisky but for Atul Gawande’s “Cost Conundrum” article in the New Yorker, in 2009 which is still required reading in medical school and MPH classes and was arguably the cornerstone of Obama health policy and the ACO movement.
Dr. Atul Gawande described overutilization and high cost of Medicare revealed by Dartmouth Atlas nationally and zeroed in on McAllen Texas. Compared to El Paso (a seemingly like comparison) McAllen was the most expensive place in America for healthcare based on Medicare claims data. Gawande highlighted the entrepreneurial, doctor-owned, Doctor Hospital at Renaissance DHR in Edinburg, TX as having fancy, modern technology while the community as a whole seemed underserved.
I have always had unease with just using Medicare data to judge costs, because there was no recognition of what I was observing on my travels, namely an enormous variation in commercial prices (not simply utilization) in hospital costs in terms of paid claims by self insured employers. Poignantly, sources at the time claimed McAllen, Texas had among the lowest commercial insurance premium places in the country. Interesting.
Dr. Gawande made a good faith attempt to include the commercial perspective in his original article; reaching out to insurers and benefit consultants who shared that utilization was similarly high in commercial and Medicare insured populations. But there was no inclusion of the costs and experience of the uninsured and Medicaid populations. Back in the day he did not have access to the commercial price data, which we now know, through more than a decade of studies, explains much more of the variation in healthcare expenditures. (The Game I have described ad nauseam elsewhere and that has been carefully documented by the folks at RAND and other researchers.
Come to McAllen
In July 2022 in San Diego, at the first fully in-person Health Forum for the AHA since Covid, I was asked to moderate the opening keynote panels. The next day I got to meet the leadership from DHR McAllen including board members, benefactor/investors and leaders who were regular attendees of the Forum and were curious to work with me as an advisor.
I tried to explain that I really don’t do projects anymore and that my business model is I come in for a day, insult people and leave. I am like Newt Gingrich, only at a lower price point.
They still wanted me to visit.
Off To McAllen
The best way to get to McAllen is the way I did it. Fly in from Manhattan. I was in New York and New Jersey for meetings and flew to McAllen via Houston on a beautiful October morning. From skyscrapers to the Rio Grande Valley and the fifth largest border conurbation of 1.5 million people.
Atul Gawande described dusty roads. I didn’t see them. Even in contrast to Manhattan, McAllen looks like most of America, endless strip malls and modern apartment and housing complexes with the occasional trailer park for “Winter Texans” from Michigan. It looks like all the Central Valley towns of California, all of Arizona, all of South Carolina, pretty much all of America. I say this as a trained urban planner.
It is not crime-ridden and dangerous or much different than most of America, except that is on the border, is 80% Spanish speaking and 40% Spanish speaking only and has high rates of poverty, despite the area’s rapid growth. Hey, Elon Musk’s Space X is moving in down the road.
How Does the Math Work?
I attended a meeting at a local bank headquarters, to meet with Board Members and DHR Senior Management. The Bank is owned by Alonzo Cantù a prominent local landowner, businessman, philanthropist, and major shareholder in the DHR. He is the driving force behind DHR and clearly dedicated to bringing world class medical care to his community. He is a powerful, forceful leader who has built a fortune in banking, real estate, and other businesses, and is a major investor in developing a sophisticated medical facility in his community. Also in the meeting was my host board member and investor Larry Safir, hospital CEO Dr. Manish Singh, a bariatric surgeon who joined from the Cleveland Clinic in 2019, Susan Turley, hospital President and the chief administrator and an industry veteran who has command over the business and financial viability of DHR. We were also joined by senior clinical and administrative leadership.
They warmly welcomed me, and we launched into a discussion.
I asked a series of questions trying to understand how things have changed over the last 13 years since Dr. Gawande’s article and how it all works (particularly the financing math).
Here is a brief summary.
In 2009, DHR was a tiny fledgling facility, really just a surgery center, whose data was not even included in the Medicare claims data underpinning the Cost Conundrum conclusions. Today they are a $750 million revenue hospital system with 350 Beds spread across a campus that is a plethora of specialty hospitals and centers as well as a broader network of 80 sites of specialty care. They are the largest doctor-owned hospital in America and the de facto safety net hospital for the greater McAllen community (a catchment area of almost 3 million people), as well as being a recently dedicated Level 1 Trauma Center. They are one of the only metropolitan areas in Texas without a district hospital (with tax raising authority), they take all comers, no questions asked about immigration status. They are unusual to say the least.
So I asked how does the math work?
In any hospital visit I always ask four simple questions
What share of patients (not revenues) is Medicare and Medicaid, over 80% they said, as is typical for many hospitals.What share are uninsured? “Only 8%”, seems low I said given on average Texas has about 20% uninsured. But as President, Susan Turley explained, if patients are sick and need care, they will find a way to draw down on state and federal supplemental funding sources such as uncompensated care pools, and provider fee-based drawdowns of Federal Medicaid funds that do not burden the state of Texas’s precious general fund coffers.What do you get paid by a typical commercial PPO contract, or from self Insured employers? Depends on the line of service, Susan Turley told me but generally between 125-150% of Medicare. “We used to be out of network for most carriers, not because we chose it, but because the plans wouldn’t include us.” Now they have contracts with practically any health plan with lives in the market. They are not playing the out of network shenanigans so beloved by private equity backed physician aggregators (until recent Surprise Billing legislation popped the bubble on that gig, sending Envision and others toward financial oblivion).Can you make money on Medicare? Yes, they said, “we can make money on most patients that we can secure payment for, and we subsidize the rest”, Turley told me.So was there rampant over utilization in the community back in the day and is there still? This is less clear. Much of the horrendous self-dealing in home health and nursing home that was in the community in 2009 (not involving DHR) seems to have abated (as Atul’s follow up visit in 2015 seemed to attest).
I was struck however, that the priority was still placed on sophisticated medical intervention for sick people not on population health, primary care infrastructure, prevention, and conservative treatment protocols. (More of which later).
When pressed on this they all believed that there was a high degree of morbidity in the community largely due to the underlying conditions of poverty, obesity, and lack of primary care coverage and services. This is consistent with the seminal work of Dr. Richard (Buz) Cooper who argued that the Dartmouth Atlas, which relies on imperfect hospital referral regions, fails to adjust for the underlying socio-demographic conditions including poverty and obesity in the community.
Further, I was reminded of the old line: “Good health is a state of incomplete diagnosis.” If you look hard enough everyone has something needing to be fixed.
“But what about the El Paso comparison” I asked. It always seemed to me the most compelling part of Atul’s analysis that a similarly situated border town further up the Rio Grande Valley did not have such high utilization rates for Medicare.
DHR folk would say that El Paso is much bigger community, and importantly has a huge military and retired military presence raising the amounts of coverage and investment in healthcare in the community, from primary care to specialty care. Again, this is consistent with Dr. Buz Cooper’s view.
Strategic Challenges
We pivoted to talk about strategic challenges.
DHR was in the midst of a strategic realignment with their current academic partner University of Texas Rio Grande Valley (UT-RGV) which was clearly top of mind. They have bold ambitions for training more doctors in their community and being a leader in clinical research and clinical trials involving majority Hispanic populations.
They were troubled by the incursions of private sector backed ACOs and primary care disrupters like Cano who were already in town and expanding. This was particularly important given that McAllen has 67% Medicare Advantage Penetration with all the national carriers seemingly competing in one of the most penetrated MA markets in the country.
They were seeking to expand into the adjacent Brownsville market and are being held up in CMS bureaucracy even though their submission is exactly within published guidelines.
But, most importantly they felt that they didn’t feel connected to national trends and policy making in DC or represented by trade associations. Doctor owned hospitals are a pariah to the AHA and even to the Federation of American Hospitals (which represents the big investor-owned chains) and the few other physician owned facilities are not organized into a coherent body.
DHR feel they can get blind sided by ideas out of DC like ACOs or CMMI pilots if they are not careful.
The Tour
DHR Board Member Larry Safir took me on a driving tour of the hospital campus and surrounding community. We drove around in a beautiful white 7 Series BMW Alpina, not a speck of dust on the car or the community.
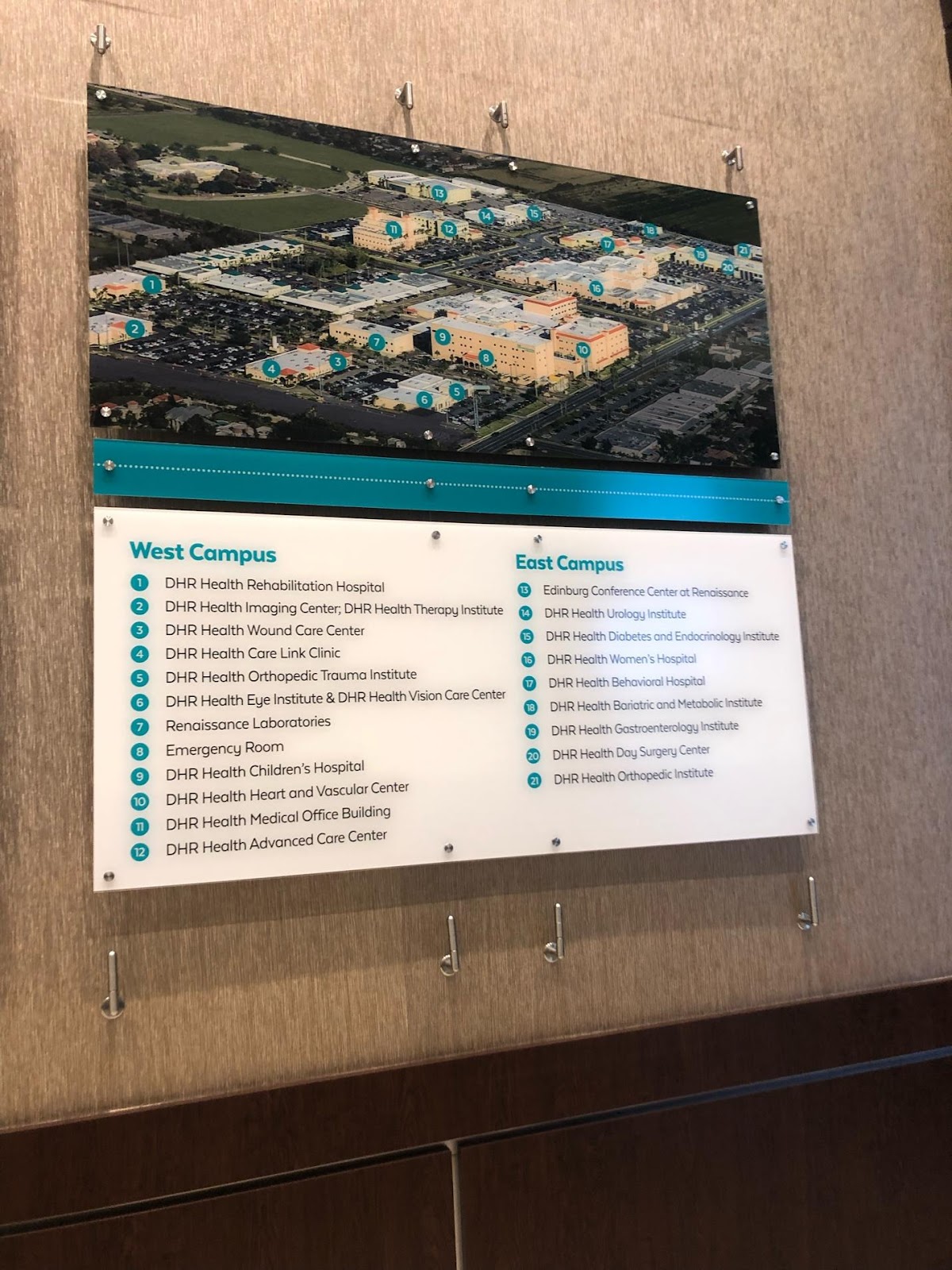
I lost count of the number of multi story specialty hospitals and institutes all in a color coordinated palette and clearly all relatively recently developed. See the Aerial shot below.
I toured the Cancer Center with its own dedicated PET scanner, advanced CT and Radiation Therapy equipment.
I toured the Women’s Hospital and NICU with Marissa Castaneda, a top executive who tore herself away from a a routine accreditation visit from the College of American Pathologist’s (their lab passed with flying colors by the way).
I am a geography major, not equipped or qualified to opine on clinical appropriateness. But I saw with my own eyes tiny 28 day old 2 lb quintuplets being cared for compassionately in a 67-bed state of the art NICU. That did not strike me as a lay person as inappropriate or excessive compared to Stanford or UCSF or any Children’s hospitals I have worked with.
The NICU is part of the Vermont Oxford Network Collaborative and is ranked in the top 5% in the world within the collaborative.
Marissa like many of the executive team is a smart, capable Latina from the community who is passionate about bringing high quality, sophisticated medical care to McAllen and is in awe of the dedication of the doctors (and investors) to that purpose. She gets emotional about the difference the care has made to her, her family, and her neighbors.
Virtually all the medical staff are owners and investors. Before DHR, Cleveland Clinic trained specialists would not be available in McAllen, now they are.
Lessons Learned
I now have a lot of friends in McAllen and appreciate their welcoming me. I learned a lot:
Good people trying to do the Right Thing for their Community. I came away with the strong impression that this was a group of dedicated people trying to do the right thing for their community and had developed a business model to make it work. Everyone seemed sincere and committed to doing the right thing as they saw it, namely bring sophisticated medical care to an underserved community.
Policy Hypocrisy of Making Physician Owned Hospitals a Pariah. Nationally, I have been arguing that we are not moving from volume to value, we are moving form volume to volume (inpatient volume to outpatient volume). Everyone is playing the volume game, employed doctors in non-profit systems are on an RVU treadmill. Singling out for profits that are doctor owned is unfair. They should be judged on a balanced scorecard (See below). Everyone in healthcare has some kind of financial motive. Why are physician- owned hospitals the orphans?
The need for a scorecard for all of healthcare beyond the drunk and the Lamppost. The original Cost Conundrum work and the pioneering Dartmouth Atlas work were important but incomplete. Like the proverbial drunk looking for his car keys under the lamppost because that is where the light is, policy wonks used Medicare data, (and Medicare FFS at that) to infer a lot of things. Much better that we build all payer balance scorecards to measure system performance (See Goldsmith and Morrison Article).
Are the Priorities Right?: Daschle’s Pyramids. Former Senator Tom Daschle who advised President Obama had a good slide he used to show of how the US healthcare systems operates in contrast to other systems around the world. As he posted in Rollcall on June 4th, 2009:
Health care in any society looks like a pyramid. The base of the pyramid comprises basic health care delivery involving wellness and prevention. It is the least costly. As we move up the pyramid, the care becomes more sophisticated and technologically advanced. At the peak are the most costly and technologically advanced applications, such as organ transplants, available in modern medicine today.
Every country begins at the base of the pyramid and works its way up until the money runs out. However, in the U.S., we start at the top of the pyramid and work our way down until the money runs out.
We might be willing to accept these prohibitively high costs if we were getting great value from the investment. But the truth is that the quality of our health care is actually declining despite of all the technological innovations that we have witnessed in recent decades.
It’s what I have written about before as The Fallacy of Excellence or more crudely, Pimp My Ride Healthcare https://ianmorrison.com/pimp-my-ride/
Put your money where your mouth is, could they take Risk? Part of me would love to see DHR take full financial risk for the population they serve. It would be magnificent if a doctor-owned, financially viable, high tech specialty healthcare system, integrated with a massive primary care and prevention base for a poor community could be created. It might be too much to ask. But the folks at DHR do appreciate the need for Daschle-like base strategy for primary care since the incursion of commercial ACOS threatens their patient flows.
The Role of Medicaid in Blue and Red States. At the meeting I came from in New Jersey, Kathleen Sibelius also spoke (Obama’s head of HHS). I asked her whether we are expecting too much of Medicaid (cover 90 million poor Americans, (including dual eligibles) cover a majority of kids and moms, be the LTC insurer for the bottom half of the income distribution and the mental health backbone). And adult Medicaid has grown 26% in enrollment during the pandemic. Secretary Sibelius did not see a prospect for sweeping national alignment in payment rates spurred by the federal government. She agreed it should happen, but the prospects are slim. And when the public health emergency ends in 2023 we may lose 15 million currently insured under Medicaid nationally as redeterminations kick in again. (2 million in California alone according to California Health Secretary Dr.Mark Ghaly at a meeting I was at just before my McAllen visit). Ghaly says they are working on ensuring coverage options through Covered California, but I am not sure there won’t be folk falling through the cracks. Ironically, California and New Jersey are Blue states with poor reimbursement but lots of Medicaid eligibles. In McAllen Texas, DHR hospital leaders say they are making money on Medicaid. Even though it is easier to get into Princeton than get a Medicaid card in Texas (certainly if you are a childless adult because they are not eligible no matter how poor). But if you get sick enough you get some care and the hospitals claim to get decent payment from state uncompensated care pools.
Californians and other liberal states take pride in lowering uninsured rates to the lowest (nationally 8%) in American history, but they have done it mainly by inadequately compensating providers and shielding governments from the rationing decisions by using private health plans as a managed care intermediary for Medicaid. And as Secretary Sibelius said in her remarks to the New Jersey audience, the Congress only cares about what they pay not what happens to employer sponsored coverage premiums or to states Medicaid reimbursement rates.
So we end up with a Medicaid Managed Care system that LA’s Martin Luther King Community Healthcare CEO Dr. Elaine Batchlor (on whose board I proudly serve) eloquently describes as “Soviet Medicine” where plans pretend to have an adequate network of specialty providers that in turn claim to see patients but often don’t.
The Liberal Fallacy and the Southern Conundrum. Texas will pay for medical care for the poor not insurance for the poor. The punchline for California is we need to raise Medicaid reimbursement rates to fulfill the promise of coverage. The punchline for Texas is end the ideological war and expand Medicaid, and if you do that it will be my true drop the mike moment.
(Aside: Self Insured employers should be fellow travelers on this road to raise Medicaid rates because they end up paying 3-400% of Medicare to Cedars and Stanford etc. to make the hospital’s math work, but having spent time with PBGH the last few years the employers think there is already too much being spent on healthcare and they want no part of higher direct taxation on employers or their high end employees, even though they are paying an indirect tax through higher commercial prices to health care providers).
Doctors Can Have Too Much Control. It is the dream of most hospital physicians to have a line-item veto over every hospital decision. I remember doing a retreat for a famous Academic Dean who told me: “I do OK in the meetings, it’s the corridors I get killed in”. I cannot imagine how difficult it is to corral a thousand or more doctor shareholders.
My McAllen visit taught me a lot about the diverse approaches to healthcare delivery and finance. I truly appreciated the opportunity to visit and the warm welcome I received. We should judge people and health systems on their behavior and outcomes not on some preconceived stylized organizational ideal. The folks in McAlllen are doing the best they can for their community.
My visit was particularly poignant as I embarked on my own recent medical adventures. More of which later.













